45 YEAR OLD MALE WITH POSTERIOR CIRCULATION STROKE
This is an online E logbook to discuss our patients' de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through a series of inputs from the available global online community of experts intending to solve those patients' clinical problems with the collective current best evidence-based inputs. This e-log book also reflects my patient-centred online learning portfolio and your valuable inputs on the comment box are welcome.
Name: Dr Sreshta J
2/2/23
45 YEAR OLD MALE CAME WITH THE
COMPLAINTS OF GIDDINESS SINCE ONE DAY
COMPLAINTS OF DOUBLE VISION SINCE MORNING
COMPLAINTS OF DIFFICULTY IN SWALLOWING SINCE MORNING
COMPLAINTS OF WEAKNESS OF LEFT LOWER LIMB AND INABILITY TO WALK SINCE MORNING
HOPI:
PATIENT WAS APPARENTLY ASYMPTOMATIC 10 YEARS AGO WHEN HE DEVELOPED FEVER FOR WHICH ROUTINE INVESTIGATIONS WERE DONE AND HE WAS DIAGNOSED WITH DIABETES MELLITUS TYPE II AND IS ON ORAL HYPOGLYCEMIC DRUGS SINCE.
3 YEARS AGO PATIENT DEVELOPED ABDOMINAL PAIN FOR WHICH HE WAS OPERATED (? APPENDICITIS) AND COLOSTOMY WAS PLACED FOR 3 MONTHS AND WAS DIAGNOSED AS HBSAG+ AND NOT ON ANY MEDICATION.
YESTERDAY IN THE EVENING HE DEVELOPED GIDDINESS. HE THOUGHT WAS DUE TO HYPOTENSION AND TOOK BUTTERMILK. THEN HE WENT TO AN RMP WHO GAVE IV FLUIDS AS HIS SYSTOLIC BP WAS 90MMHG, WITH WHICH GIDDINESS DIDN'T SUBSIDE. HE HAD VOMITINGS 1 EPISODE - FOOD PARTICLES AS CONTENT, NON BILIOUS, NON PROJECTILE, NON BLOOD STAINED
THEN HE WENT HOME AT 10 PM AND SLEPT.
HE TRIED TO WAKE UP AT 5AM , HE COULDN'T DUE TO WEAKNESS OF LEFT LOWER LIMB AND SEVERE GIDDINESS. HE ALSO DEVELOPED DIFFICULTY IN SWALLOWING (SOLIDS>LIQUIDS) AND DIPLOPIA AND WAS TAKEN TO LOCAL HOSPITAL IN THE MORNING AT 10AM. AN MRI WAS DONE AND HE WAS FOUND TO HAVE ACUTE INFARCTS IN LEFT MEDULLA AND INFERIOR CEREBELLAR HEMISPHERE. THEREFORE HE WAS REFERRED HERE FOR FURTHER MANAGEMENT
PAST ILLNESS:
KNOWN CASE OF DIABETES MELLITUS TYPE II SINCE 10 YEARS AND ON ORAL HYPOGLYCEMIC DRUGS (UNKNOWN)
OPERATED FOR ? APPENDICITIS 3 YEARS AGO AND COLOSTOMY WAS PLACED FOR 3 MONTHS AND WAS DIAGNOSED AS HBSAG+ AND NOT ON ANY MEDICATION.
NOT A KNOWN CASE OF HYPERTENSION, ASTHMA, CAD, CVD
PERSONAL HISTORY:
DIET: MIXED
APPETITE: DECREASED
BOWEL AND BLADDER MOVEMENTS: REGULAR
SLEEP: ADEQUATE
ADDICTIONS: ALCOHOLIC SINCE 3 YEARS ( BRANDY)
CIGARETTE SMOKING SINCE 15 YEARS
KHAINI CHEWING SINCE 20 YEARS



ON EXAMINATION:
PATIENT IS CONSCIOUS COHERENT AND COOPERATIVE
GENERAL EXAMINATION:
NO PALLOR ICTERUS CYANOSIS CLUBBING LYMPHADENOPATHY EDEMA
VITALS:
BP- 90/60 MMHG
PR- 59 BPM
RR- 18 CPM
SPO2- 98% @RA
GRBS- 283MG/DL
CVS- S1 S2 HEARD. NO MURMURS
RS- BAE+
P/A- SOFT, NON TENDER
CNS-
GCS- E4VM6
RT LT
TONE UL N N
LL N N
POWER UL 5/5 5/5
LL 5/5 4/5
REFLEXES BICEPS + ++
TRICEPS + ++
SUPINATOR ++ ++
KNEE + +
ANKLE - -
PLANTARS- MUTE FLEXOR
PROVISIONAL DIAGNOSIS:
POSTERIOR CIRCULATION STROKE WITH ACUTE INFARCT IN LEFT MEDULLA AND INFERIOR CEREBELLAR HEMISPHERE.
HEPATITIS B POSTIVE SINCE 3 YEARS
WITH KNOWN CASE OF DIABETES MELLITUS TYPE II SINCE 10 YEARS (ON ORAL HYPOGLYCEMIC DRUGS)
TREATMENT:
RT FEEDS- 100ML MILK 4TH HOURLY
50ML WATER 2ND HOURLY
T. ECOSPRIN 75MG RT OD
T. CLOPITAB 70MG RT OD
T. ATORVAS 10MG RT HS
T. BACLOFEN 10MG RT OD
INJ PROMETHAZINE 25MG IM BD
INJ HUMAN ACTRAPID INSULIN SC TID ACC TO SLIDING SCALE
INJ PAN 40MG IV OD
INJ ZOFER 4MG IV BD
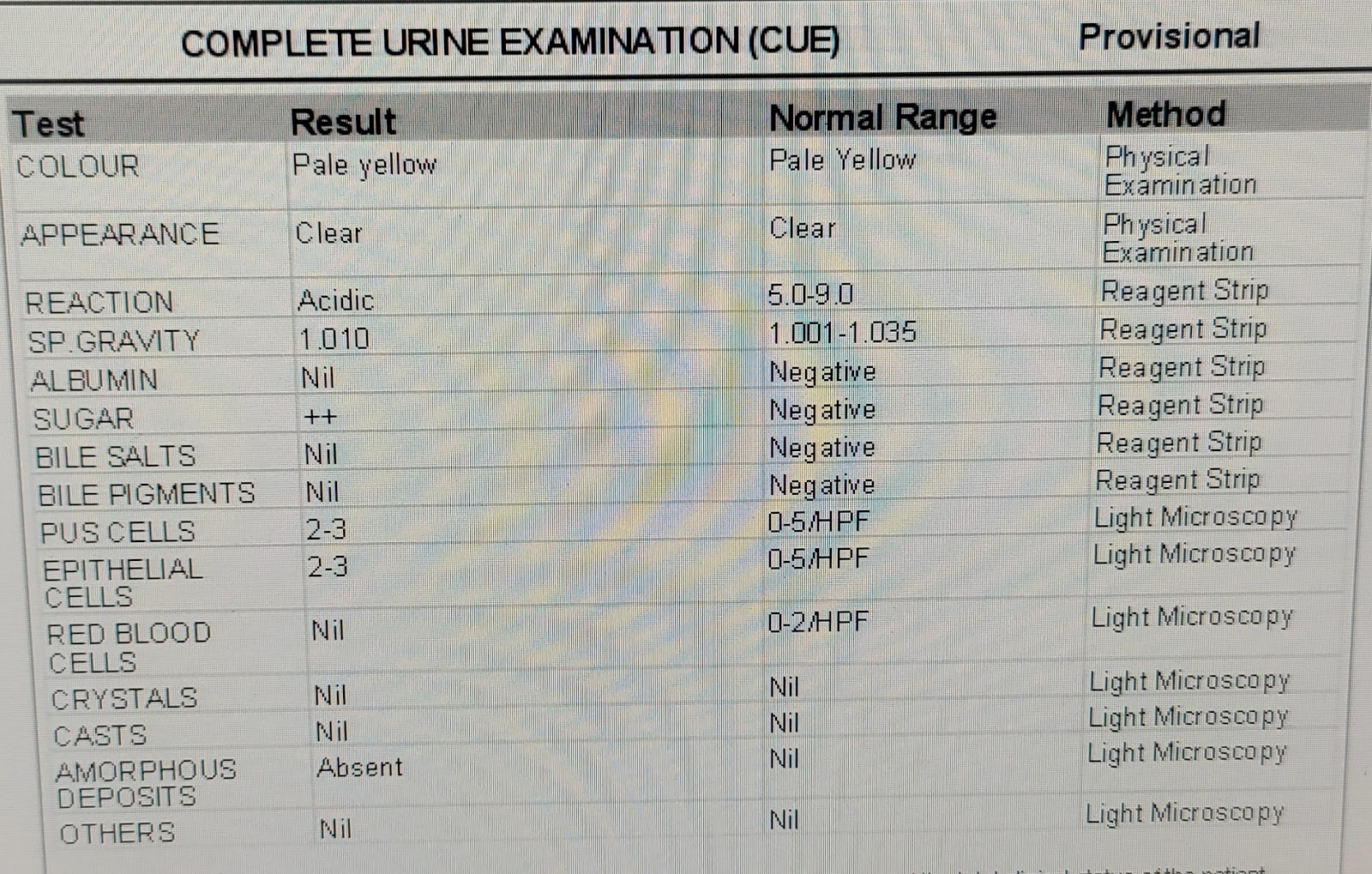
INVESTIGATIONS:
AT ADMISSION:














4/2/23








5/2/23



6/2/23

3/2/23 SOAP NOTES
GM UNIT 4
ICU BED 1
DR. SUSMITHA (SR)
DR. CHANDANA (PGY3)
DR. HARIPRIYA (PGY2)
DR. GOVERDHINI (PGY1)
DR. SRESHTA (INTERN)
S-
C/O VOMITINGS - SUBSIDED
C/O GIDDINESS
C/O DOUBLE VISION
O-
BP- 90/60MMHG
PR- 65BPM
RR- 12CPM
SPO2- 98% @RA
TEMP- 99.2F
GRBS- 214MG/DL
CVS- S1 S2 +
RS- BAE+
PA- SOFT AND NON TENDER
CNS-
GCS- E4V5M6
RT LT
TONE UL N N
LL N N
POWER
UL 5/5 5/5
LL 5/5 4/5
REFLEXES
BICEPS + ++
TRICEPS + ++
SUPINATOR ++ ++
KNEE + +
ANKLE - -
PLANTARS-
MUTE FLEXOR
NYSTAGMUS-
HORIZONTAL+
VERTICAL+
A-
POSTERIOR CIRCULATION STROKE WITH ACUTE INFARCT IN LEFT MEDULLA AND INFERIOR CEREBELLAR HEMISPHERE.
HEPATITIS B POSTIVE SINCE 3 YEARS
WITH KNOWN CASE OF DIABETES MELLITUS TYPE II SINCE 10 YEARS (ON ORAL HYPOGLYCEMIC DRUGS)
P-
RT FEEDS- 100ML MILK 4TH HOURLY
50ML WATER 2ND HOURLY
T. ECOSPRIN 75MG RT OD
T. CLOPITAB 75MG RT OD
T. ATORVAS 10MG RT HS
T. BACLOFEN 10MG RT OD
INJ HUMAN ACTRAPID INSULIN SC TID ACC TO SLIDING SCALE
INJ PAN 40MG IV OD
INJ ZOFER 4MG IV BD
4/2/23 SOAP NOTES
GM UNIT 4
ICU BED 1
DR. SUSMITHA (SR)
DR. CHANDANA (PGY3)
DR. HARIPRIYA (PGY2)
DR. GOVERDHINI (PGY1)
DR. SRESHTA (INTERN)
S-
C/O VOMITINGS - SUBSIDED
C/O GIDDINESS
C/O DOUBLE VISION
O-
BP- 90/60MMHG
PR- 68BPM
RR- 20CPM
SPO2- 97% @RA
GRBS- 117MG/DL
CVS- S1 S2 +
RS- BAE+
PA- SOFT AND NON TENDER
CNS-
GCS- E4V5M6
RT LT
TONE UL N N
LL N N
POWER
UL 5/5 5/5
LL 5/5 4/5
REFLEXES
BICEPS + ++
TRICEPS + -
SUPINATOR + +
KNEE + +
ANKLE - -
PLANTARS-
EXTENSOR FLEXOR
A-
POSTERIOR CIRCULATION STROKE WITH ACUTE INFARCT IN LEFT MEDULLA AND INFERIOR CEREBELLAR HEMISPHERE.
HEPATITIS B POSTIVE SINCE 3 YEARS
WITH KNOWN CASE OF DIABETES MELLITUS TYPE II SINCE 10 YEARS (ON ORAL HYPOGLYCEMIC AGENTS)
P-
RT FEEDS- 100ML MILK 4TH HOURLY
50ML WATER 2ND HOURLY
T. ECOSPRIN 75MG RT OD
T. CLOPITAB 75MG RT OD
T. ATORVAS 10MG RT HS
T. BACLOFEN 10MG RT OD
INJ PROMETHAZINE 25MG IM BD
INJ HUMAN ACTRAPID INSULIN SC TID ACC TO SLIDING SCALE
INJ PAN 40MG IV OD
INJ ZOFER 4MG IV BD
7/1/23 SOAP NOTES
GM UNIT 4
WARD
DR. SUSMITHA (SR)
DR. CHANDANA (PGY3)
DR. HARIPRIYA (PGY2)
DR. GOVERDHINI (PGY1)
DR. SRESHTA (INTERN)
S-
C/O VOMITINGS - SUBSIDED
C/O GIDDINESS ON WALKING
C/O GENERALISED WEAKNESS
C/O HICCUPS
C/O TINGLING SENSATION OVER LEFT UPPER LIMB
O-
PT IS CONSCIOUS COHERENT AND COOPERATIVE
BP- 90/50MMHG
PR- 72BPM
RR- 16CPM
SPO2- 98% @RA
GRBS- 239MG/DL
CVS- S1 S2 +
RS- BAE+
PA- SOFT AND NON TENDER
CNS-
GCS- E4V5M6
RT LT
TONE UL N N
LL N N
POWER
UL 5/5 4/5
LL 5/5 4/5
REFLEXES
BICEPS + +
TRICEPS + -
SUPINATOR - -
KNEE - -
ANKLE - -
PLANTARS-
FLEXION FLEXION
A-
POSTERIOR CIRCULATION STROKE WITH ACUTE INFARCT IN LEFT MEDULLA AND INFERIOR CEREBELLAR HEMISPHERE.
HEPATITIS B POSTIVE SINCE 3 YEARS
WITH KNOWN CASE OF DIABETES MELLITUS TYPE II SINCE 10 YEARS (ON ORAL HYPOGLYCEMIC AGENTS)
P-
T. ECOSPRIN 75MG PO OD
T. CLOPITAB 75MG PO OD
T. ATORVAS 10MG PO HS
T. BACLOFEN 10MG PO BD
T PROMETHAZINE 25MG PO BD
T GLIMI M1 PO OD
8/1/23 SOAP NOTES
GM UNIT 4
WARD
DR. SUSMITHA (SR)
DR. CHANDANA (PGY3)
DR. HARIPRIYA (PGY2)
DR. GOVERDHINI (PGY1)
DR. SRESHTA (INTERN)
S-
C/O VOMITINGS - SUBSIDED
C/O GIDDINESS ON WALKING
C/O GENERALISED WEAKNESS
C/O HICCUPS
C/O TINGLING SENSATION OVER LEFT UPPER LIMB
STOOLS PASSED
O-
PT IS CONSCIOUS COHERENT AND COOPERATIVE
BP- 90/60MMHG
PR- 78BPM
RR- 17CPM
SPO2- 97% @RA
GRBS- 249MG/DL
CVS- S1 S2 +
RS- BAE+
PA- SOFT AND NON TENDER
CNS-
GCS- E4V5M6
RT LT
TONE UL N N
LL N N
POWER
UL 5/5 4/5
LL 5/5 4/5
REFLEXES
BICEPS + +
TRICEPS + -
SUPINATOR - -
KNEE - -
ANKLE - -
PLANTARS- FLEXION FLEXION
A-
POSTERIOR CIRCULATION STROKE WITH ACUTE INFARCT IN LEFT MEDULLA AND INFERIOR CEREBELLAR HEMISPHERE.
HEPATITIS B POSTIVE SINCE 3 YEARS
WITH KNOWN CASE OF DIABETES MELLITUS TYPE II SINCE 10 YEARS (ON ORAL HYPOGLYCEMIC AGENTS)
P-
T. ECOSPRIN 75MG PO OD
T. CLOPITAB 75MG PO OD
T. ATORVAS 10MG PO HS
T. BACLOFEN 10MG PO BD
T PROMETHAZINE 25MG PO BD
T GLIMI M1 PO OD


Comments
Post a Comment